In this “Ask Me Anything” (AMA) episode, Peter and Bob discuss the longevity benefits from greater cardiorespiratory fitness (CRF) and greater muscle mass and strength. Conversely, they dive deep into the literature showing a rapid increase in morbidity and mortality risk as fitness levels decline with age. They also try to tease out the relative contributions of CRF, muscle mass, and strength. Additionally, they discuss the impact of fasting on muscle mass, the potential tradeoffs to consider, and finish by discussing why it’s critical to maximize your fitness level.
If you’re not a subscriber and listening on a podcast player, you’ll only be able to hear a preview of the AMA. If you’re a subscriber, you can now listen to this full episode on your private RSS feed or on our website at the AMA #27 show notes page. If you are not a subscriber, you can learn more about the subscriber benefits here.
We discuss:
- VO2 max and its association with cardiorespiratory fitness [2:45];
- Changing mortality risk based on VO2 max and cardiorespiratory fitness [7:45];
- The profound impact of improving cardiorespiratory fitness [15:15];
- Muscle mass, function, and loss with aging: how it’s defined, measured, and the cutoff points for sarcopenia [25:00];
- Increasing mortality risk associated with declining muscle mass and strength [40:00];
- Muscle size vs. strength—which has the bigger impact on mortality risk? [58:00];
- Evaluating the cumulative impact of cardiorespiratory fitness and muscular strength on mortality risk when put together [1:03:30];
- Investigating the rising incidence in deaths from falls, and what role Alzheimer’s disease might play [1:09:00];
- The impact of fasting on muscle mass and the potential tradeoffs to consider [1:14:30];
- The critical importance of working to maintain muscle mass and strength as we age [1:20:30]; and
- More.
Get Peter’s expertise in your inbox 100% free.
Sign up to receive An Introductory Guide to Longevity by Peter Attia, weekly longevity-focused articles, and new podcast announcements.
VO2 max and its association with cardiorespiratory fitness [2:45]
Overview of question being asked today: Does better cardiorespiratory fitness lead to less mortality and does lower cardiorespiratory fitness lead to higher mortality? Or is it at least associated?
Common terms:
- Most common thing in the literature is either METs, metabolic equivalents or VO2 max
- For a VO2 max test…
- You are hooked up to an indirect calorimeter—a device that provides complete occlusion around your mouth and your nose so you’re only breathing through your mouth
- The device has two sensors on it
- One sensor measures the concentration of oxygen that is being expelled
- The other one is also measuring the concentration of carbon dioxide that’s expelled.
- Because we know the concentration of oxygen and CO2 on the way in, by knowing what comes out and obviously oxygen will be lower, CO2 will be higher, we know how much carbon dioxide was produced and how much oxygen was consumed
- Knowing those two things gives you a “flow rate” — VO2 and a VCO2
- This can tell you how much energy you’re utilizing via something called the Fick principle
- Total energy consumption is ~3.94 times VO2, and ~1.11 times VCO2 at any point in time
- For instance, for this minute VO2 was X, VCO2 was Y, then you apply it to that equation and it will tell you that you were utilizing, say, 10 kilocalories per minute which would be 600 kilocalories per hour
- During Peter’s zone 2 exercise, it tends to be about 780 kilocalories per hour
- But now what we’re talking about is something different which is… what is the maximum utilization of oxygen?
- If you make somebody work harder and harder and harder, at some point they will reach a maximum at which point, they can no longer utilize more oxygen
⇒ As to the “why” they can’t utilize more oxygen, see the Alex Hutchinson podcast
- We talked about some of the alveolar limitations, how much of that is being limited at the gas exchange surface versus
- How much of that is being limited in the muscle.
- But regardless of which of those it is—and it’s possible it’s a combination or it’s possible that at low levels of fitness it’s more in the muscle, and at high levels of fitness, it might be more in the lung—but that number is the VO2 max
When you’re doing the test, it’s measured typically in liters per minute
- then we normalize it by body weight to get milliliters per kilogram per minute
- The fittest of the fit are going to be north of 80
- But what does that mean?
- It means they are north of 80 milliliters of oxygen per kilogram per minute
- The highest ever recorded VO2 max was a cyclist named Oskar Svendsen who measured about 96
- Any sort of elite cardiac type athlete, a runner, cyclist, rower, those sorts of athletes, they’re generally going to be above 70
Changing mortality risk based on VO2 max and cardiorespiratory fitness [7:45]
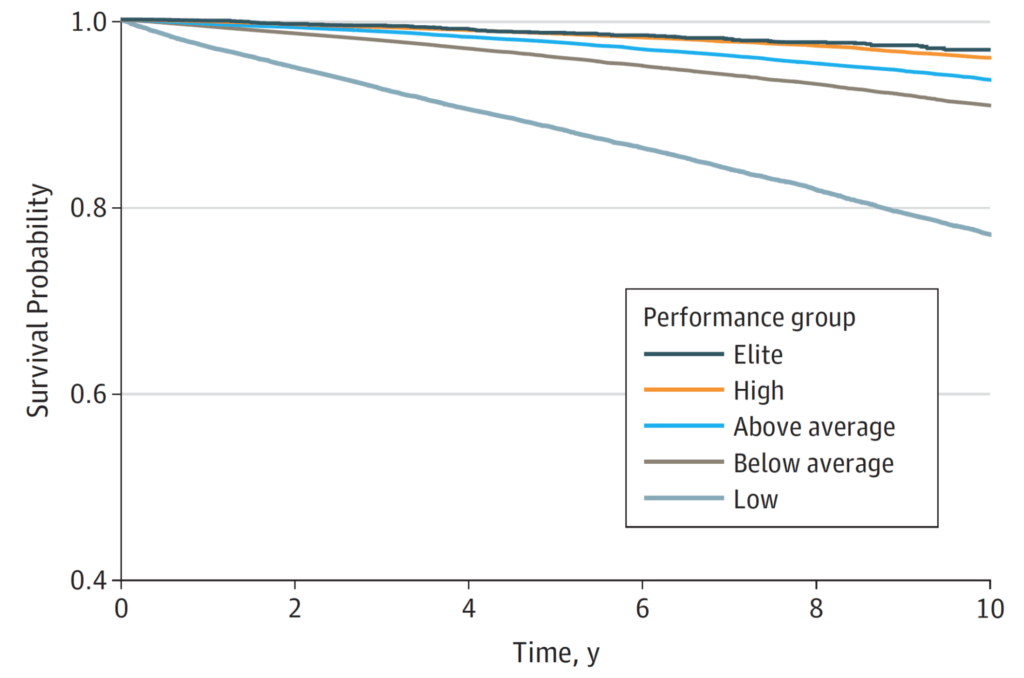
Figure 1. Patient survival by performance group. (Mandsager et al., 2018)
Overview of the experiment:
- A group of people that were 53 years old on average
- Ran them through a VO2 max test and then it ranked them
- Low were people who scored in the bottom 25th percentile
- Below average was the 25th to 50 percentile
- 50 to 75th percentile was above average
- High was 75th to maybe 95th
- Elite was just that top 5%.
- NOTE: Each of these levels do NOT represents 20% of the population
- A total of 122,000 patients
- The low, below average, above average, and high have about 30,000 participants in each one of those groups
- And then the elite group has a little over 3,500
Results:
- Looking at all-cause mortality there’s a pretty clear trend
- The two things that stand out are,
- i) there’s kind of a monotonic relationship between fitness and mortality
- ii) By far the biggest gap is between the people in the bottom 25%. Which are categorized as low fitness, and basically everyone above them.
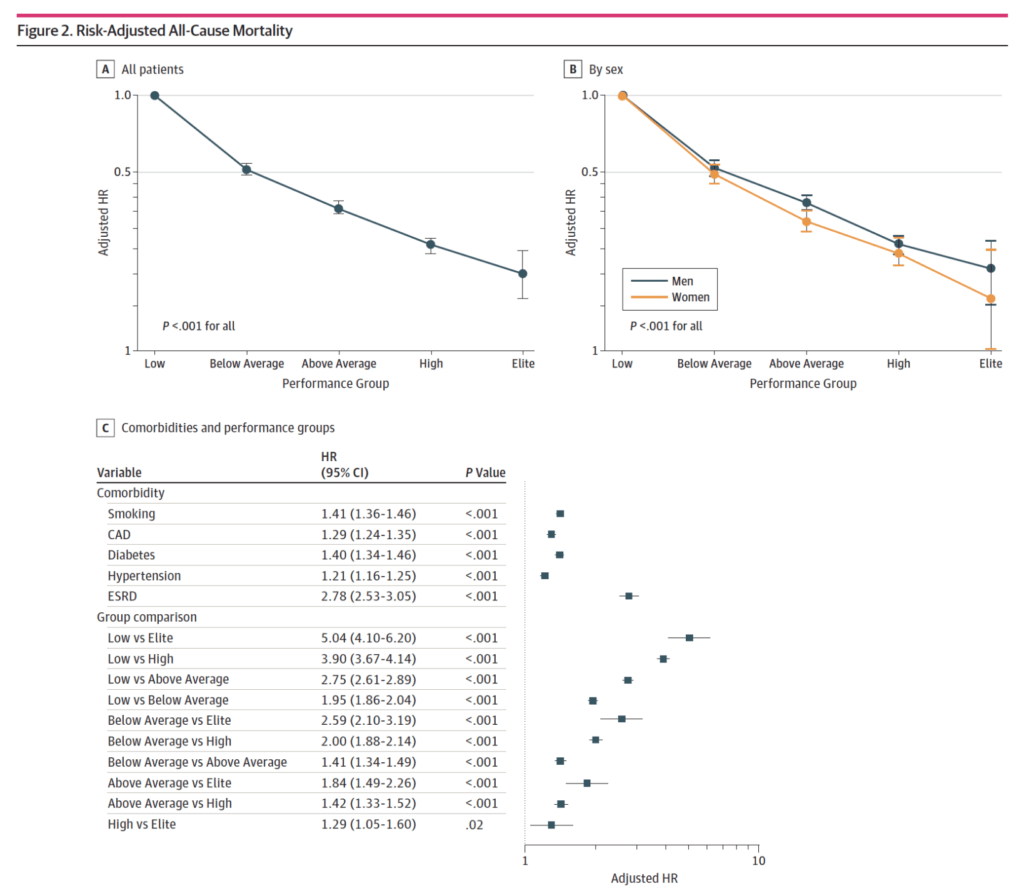
Figure 2. Risk-adjusted all-cause mortality. (Mandsager et al., 2018).
When sort of lumping everyone in together, male and female, if you have low fitness and then comparing it to everybody else, what’s the risk reduction?
If you go from low to below average, to above average, to high to elite, you can see what is the hazard ratio
Important stats
- Going from just being low to being below average is a 50% reduction in mortality over a decade
- If you then go from low to above average, it’s about a 60% or 70% reduction in mortality
- Then it just continues monotonically to increase
- The lowest improvement is going from high to elite—”That doesn’t buy you a whole heck of a lot. It is still statistically significant.”
- To see that you have to look at Table C
- remember, the hazard ratio for mortality is the reciprocal of the hazard ratio of risk reduction
- Tables A and C are basically showing you similar things in the group comparison
Here’s what’s interesting…
- If you compare someone of low fitness to elite, it is a five fold difference in mortality over a decade
- They put this in the context of other things that we commonly understand as being problematic for mortality… Namely, smoking, coronary artery disease, Type 2 diabetes, hypertension, and end-stage renal disease
- That’s a 41% increase in mortality over the decade
- Coronary artery disease, 29%.
- Diabetes, 40%.
- High blood pressure, 21%.
- End-stage renal disease, about 180% increase in mortality
- But now when you compare that to the differences in these fitness levels, it gives you a greater appreciation for how much improvement in mortality comes from improving your fitness
- If you look at the biggest driver of mortality, which would be end-stage renal disease in this cohort, it’s the same as going from low cardiorespiratory fitness to above average cardiorespiratory fitness
- So going from the bottom 25th percentile to being in the 50th to 75th percentile… “which is a totally achievable feat”
{end of show notes preview}
Would you like access to extensive show notes and references for this podcast (and more)?
Check out this post to see an example of what the substantial show notes look like. Become a member today to get access.